3-D musculoskeletal ultrasound as an adjunctive measure to clinical gait analysis
A.P. Shortland, N.R. Fry and M. Gough
Gait Laboratory, Guy's Hospital, London, United Kingdom
Gait analysis is used for treatment decision-making and assessment of intervention in cerebral palsy, but its power is limited by the variability in, and interpretation of, results. The clinician needs to distinguish the contributions made by muscular weakness, altered neurology and deformity, but often many conclusions can be drawn on the basis of any one set of data. There is a need for complementary investigations, to improve the specificity of gait analysis; one of these may be musculoskeletal ultrasound imaging.
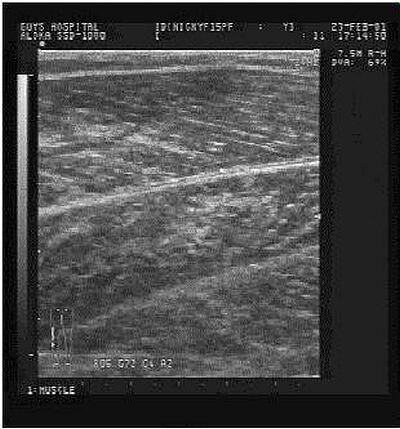
Ultrasound devices transmit high frequency sound waves. Echoes are received from boundaries between tissues of different acoustic impedance. In this way, bone, blood, myofibrillar and connective tissue can be distinguished within an image. Recently, researchers have begun to investigate muscle architecture (Figure 1) with ultrasound, to assess the effects of immobilisation after cruciate ligament surgery [1] and strengthening regimes [2]. Shortland et al. [3] have evaluated the architecture of gastrocnemius in cerebral palsy, with implications for our understanding of muscle contracture in this group. While informative, 2-D studies are limited because the complete muscle morphology cannot be detailed.
Figure 1. 2-D ultrasound image of the medial gastrocnemius.
Freehand 3-D ultrasound systems can be used to visualize the gross structure of muscles. Generally, such systems consist of a magnetic positional sensor attached to a B-mode ultrasound probe. The video output of the ultrasound scanner, and near-synchronous positional information, are combined to produce a collection of non-uniformly orientated image slices. These can be reconstructed into a regularly spaced three dimensional matrix. Different views of the gross structure of the muscle under study can be obtained by "reslicing" the volume (Figure 2).
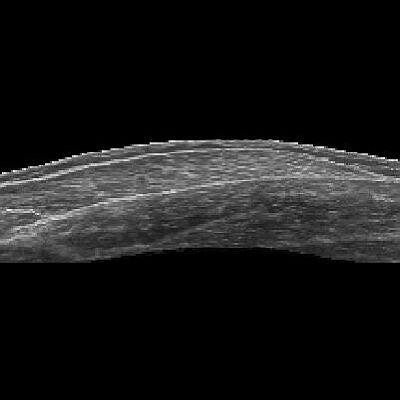
Figure 2. Longitudinal view (20 cm) of a 3-D ultrasound image.
3-D ultrasound systems do not require magnetic positional sensors. We have used an optical motion analysis system to track the position of an ultrasound probe and collect images from a scanner on a frame-grabber [4]. With this device, we have measured gastrocnemius muscle belly length in normally-developing adults and children, and in children with spastic diplegia. Derived muscle dimensions may be very useful to the clinician who wishes to assess muscle deformity and mechanical capacity [5] before deciding upon an intervention, such as musculotendinous lengthening, splinting or tendon transfers. What is more, the effect of focal interventions on muscle morphology can be evaluated.
References
Paper presented at Measuring Behavior 2002, 4th International Conference on Methods and Techniques in Behavioral Research, 27-30 August 2002, Amsterdam, The Netherlands